Assessment of Vocal Hyperfunction

Voice abnormalities in children are often first detected by family members or school teachers, however, before the child can be referred for voice therapy, they must complete a voice screening by an SLP. A screening is a quick test that enables the SLP to determine whether or not the child does actually have a voice disorder. The screening does not provide the clinician with details as to the nature or cause of the disorder. If the child’s voice is found to be abnormal based on the screening, then the SLP will refer the child for further evaluation, including a medical evaluation by an otolaryngologist or ENT. A comprehensive voice evaluation is required in order to ensure that the client gets the proper treatment and voice therapy they require (Boone, 2010). An evaluation based solely on the clinician’s perception of the client’s voice is insufficient, as many voice disorders present with identical symptoms, yet have totally different underlying causes (Lee, Stemple, Glaze, & Kelcher, 2004). For example, hoarseness can be an indication of vocal hyperfunction caused by excessive yelling, yet can also be indicative of contact ulcers on the vocal folds (Boone, 2010). Successful voice therapy largely depends on treating the cause of the disorder and therefore, the assessment procedures are an extremely integral aspect of voice rehabilitation (Oates & Winkworth, 2008).
Voice Screening
A screening tool is used to quickly identify children with voice disorders. Although it is usually individuals other than the SLP that first identify a voice problem in a child, it is routine that the child be screened by a certified SLP who is knowledgeable and qualified to make accurate judgments regarding the normalcy of voice (Lee et al., 2004). SLPs are currently working on implementing mass voice screenings in schools to allow for early identification of childhood voice disorders, such as vocal hyperfunction. Each screening takes only a few minutes to complete and is used to measure various aspects of voice. If the child does not pass the voice screening, then they will be referred for a complete voice evaluation (Boone, 2010).
The following voice screening tools are easy-to-administer and are commonly used in screening children:
A screening tool is used to quickly identify children with voice disorders. Although it is usually individuals other than the SLP that first identify a voice problem in a child, it is routine that the child be screened by a certified SLP who is knowledgeable and qualified to make accurate judgments regarding the normalcy of voice (Lee et al., 2004). SLPs are currently working on implementing mass voice screenings in schools to allow for early identification of childhood voice disorders, such as vocal hyperfunction. Each screening takes only a few minutes to complete and is used to measure various aspects of voice. If the child does not pass the voice screening, then they will be referred for a complete voice evaluation (Boone, 2010).
The following voice screening tools are easy-to-administer and are commonly used in screening children:
- The Boone Voice Program for Children Voice Screening Form: This screening tool is appropriate for children of all ages and uses an easy three-point scoring system to rate voices in areas of respiration, phonation, and resonance. The clinician listens to natural voice samples of the child and determines whether the child's voice is normal for their age, gender and race. If the child's voice is found to be abnormal in any area, then they are seen again within a few weeks for a followup screening. If they are still found to display deviant voice features the second time around, then they are referred for a medical and voice evaluation (Boone, 2010).
- The Quick Screen for Voice: As per the name, this voice screening tool can be administered in as little as 5-10 minutes and is suitable for both children and adults. It too, assesses the areas of respiration, phonation, and resonance, as well as vocal flexibility. A checklist, organized according to these four areas, is used for the clinician to mark down any notable observations. If one or more areas of voice production is found to be abnormal, then the child fails the screening and is referred for a complete evaluation (Lee et al., 2004).
Evaluation Procedures
Once the child has been identified as having a voice disorder, the evaluation process begins. Evaluation of vocal hyperfunction in children requires a multidisciplinary approach. A voice trained SLP will usually work together with a pediatric otolaryngologist (ENT) in order to reach a diagnosis that represents all medical and perceptual aspects of the child's disorder. Other medical professionals can be consulted along the way as a need by need basis (Theis, 2010),
A complete pediatric voice evaluation can be broken down into the following components which will all be discussed in detail:
Case History: The first step of a voice assessment, and really any assessment for that matter, is to obtain a thorough case history from the child and their parents/caregivers. The case history should be detailed and include information regarding the description of the problem and its probable cause, the onset and duration of the problem, the client's medical history, as well as a detailed description of the client's daily voice use (or misuse) patterns (Boone, 2010). The information obtained from a case history can provide valuable insight as to what the cause of the disorder might be and aid in differential diagnosis. For example, if a child complains of hoarseness that is worse in the mornings than at night, then gastroesophageal reflux would be considered (Theis, 2010). Sometimes, parents may be asked to fill out a questionnaire or a checklist in addition to the interview with the clinician (Boone, 2010). Sample questions can be seen in the "Functional Indicators Checklist" attached below. This particular questionnaire primarily focuses on the child's experiences on using their voice in their everyday lives, as well as some medical history questions (Lee et al., 2004).
Once the child has been identified as having a voice disorder, the evaluation process begins. Evaluation of vocal hyperfunction in children requires a multidisciplinary approach. A voice trained SLP will usually work together with a pediatric otolaryngologist (ENT) in order to reach a diagnosis that represents all medical and perceptual aspects of the child's disorder. Other medical professionals can be consulted along the way as a need by need basis (Theis, 2010),
A complete pediatric voice evaluation can be broken down into the following components which will all be discussed in detail:
- Thorough Case History
- Oral-Motor Examination
- Auditory-Perceptual Assessment
- Instrumental Analyses
- Laryngoscopy (Boone, 2010)
Case History: The first step of a voice assessment, and really any assessment for that matter, is to obtain a thorough case history from the child and their parents/caregivers. The case history should be detailed and include information regarding the description of the problem and its probable cause, the onset and duration of the problem, the client's medical history, as well as a detailed description of the client's daily voice use (or misuse) patterns (Boone, 2010). The information obtained from a case history can provide valuable insight as to what the cause of the disorder might be and aid in differential diagnosis. For example, if a child complains of hoarseness that is worse in the mornings than at night, then gastroesophageal reflux would be considered (Theis, 2010). Sometimes, parents may be asked to fill out a questionnaire or a checklist in addition to the interview with the clinician (Boone, 2010). Sample questions can be seen in the "Functional Indicators Checklist" attached below. This particular questionnaire primarily focuses on the child's experiences on using their voice in their everyday lives, as well as some medical history questions (Lee et al., 2004).
| Functional Indicators Checklist.pdf |

Oral-Motor Examination: An oral-motor examination is a routine part of a voice assessment. It involves the clinician visually examining the structures used in producing speech, such as the face, oral and nasal cavities, pharynx, larynx, and respiratory systems for any visible abnormalities. In the case of vocal hyperfunction, the clinician would be looking for signs of excess muscle tension in the neck, as well as abnormal or excessive movements of the larynx during various pitches. These characteristics of hyperfunction can be visually observed during an oral-motor examination. It is important to note, however, that the majority of problems associated with vocal hyperfunction, such as vocal chord abnormalities, can not be visually detected through the oral-motor examination and require laryngoscopy, which is discussed below (Boone, 2010).

Auditory-Perceptual Assessment: The auditory-perceptual assessment involves describing the voice, solely by listening. SLPs who specialize in voice disorders are specially trained to pick up on, and describe the various vocal characteristics present in a disordered voice (Williamson, 2008). Although voice perception is subjective, the auditory-perceptual assessment is nevertheless a critical component of the voice evaluation because it provides the SLP with the necessary information to determine whether or not the person has a voice disorder and if so, what areas to target through voice therapy. Various protocols and voice scales have been developed to offer clinicians a more standardized (specified and consistent) approach to evaluating and documenting auditory-perceptual judgments of vocaal quality (Kempster, Gerrat, Verdolini Abbott, Barkmeier-Kraemer, & Hillman, 2009). Some of the commonly used protocols include the following:
In children with vocal hyperfunction, the following characteristics are usually observed during an auditory perceptual assessment: dysphonia (hoarse, breathy, or rough voice), voice and pitch breaks, excessively loud voice, intermittent aphonia, and an effortful/strained voice (Glaze, 1996).
- The Buffalo III Voice Profile- Developed in 1987, this protocol measures laryngeal tone, pitch, loudness, nasal and oral resonance, breath supply, muscles, voice abuse, rate, speech anxiety, speech intelligibility and an overall voice rating. It is scored using a 5-point scale ranging from 1=normal to 5=very severe (Williamson, 2008).
- The GRBAS Scale- This scale was developed in 1981 and was designed specifically to evaluate voice quality. It measures: Grade (the overall severity of voice abnormality), Roughness, Breathiness, Aesthenia (voice weakness, and Strain. Each parameter is rated using a 4-point scale ranging from 0=normal to 3=severe (Williamson, 2008)..
- The CAPE-V (Consensus Auditory Perceptual Evaluation of Voice)- This scale was developed most recently by a special division of ASHA (American Speech-Language and Hearing Association). The SLP will rate six aspects of voice including overall severity, roughness, breathiness, strain, pitch and loudness, by making a mark on a 100ml line (left end of line represents normal function). The CAPE-V is unique because of its use of visual analog scales and because of the fact that it is unanchored (Boone, 2010).
In children with vocal hyperfunction, the following characteristics are usually observed during an auditory perceptual assessment: dysphonia (hoarse, breathy, or rough voice), voice and pitch breaks, excessively loud voice, intermittent aphonia, and an effortful/strained voice (Glaze, 1996).

Instrumental Analyses: Today, with major advances in technology, there are many instrumental techniques available to aid clinicians in evaluating voice. An instrumental analysis can include an acoustic analysis and aerodynamic measurements.
- Acoustic Analysis: This is kind of an "objective" counterpart to the auditory-perceptual evaluation and it is often included as part of a voice assessment. An acoustic analysis measures fundamental frequency, intensity, perturbation, sound spectropraphy and harmonics to noise ratio using a computerized program designed to do so, such as the Computerized Speech Lab. The client is usually asked to perform a variety of tasks such as sustain a vowel, engage in natural conversation, and read a passage (if child can read). All responses are recorded and converted into a sound waveform and spectrograph, allowing the clinician to measure the different features mentioned above (Williamson, 2008). Here is just one sample of an Acoustic analysis protocol (Brindle, 2012).
| cd_508_instrumental_dx_form_rev.pdf |
- Aerodynamic Measures: These are used to reveal information about the valving activity of the larynx and measure the following: lung volumes and capacities, air pressure, airflow, laryngeal resistance, and durational measures such as maximum phonation duration (Boone, 2010). Obtaining these measurements, however, can be challenging in the pediatric population (Theis, 2010).
Laryngoscopy: Endoscopic examination for laryngeal observation is essential in diagnosing pediatric voice disorders in order to rule out or identify any laryngeal pathology. An accurate diagnosis is otherwise virtually impossible (Theis, 2010). ASHA states that no person with voice disorders shall receive voice therapy until they have been examined by a physician, usually an ENT or otolaryngologist. This is important because as mentioned previously, voice therapy can only be effective when there are no other underlying medical conditions causing the voice disorder. In the case of vocal hyperfunction, usually a behavioral treatment approach is taken that teaches the child how to use better voicing habits however, if there is some medical condition that is causing the hyperfunction, then the medical issue will have to be resolved first before any voice therapy can be effective. A laryngeal examination will determine the etiology of the voice disorder and only then can a successful treatment plan be put into action (Boone, 2010).
There are different methods of laryngeal examination. Each paragraph below gives a brief description of each method as well as lists their various pros and cons.
There are different methods of laryngeal examination. Each paragraph below gives a brief description of each method as well as lists their various pros and cons.
-Mirror Laryngoscopy:
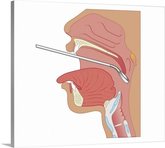
A small mirror on a handle is placed in the back of the clients mouth and angled so that the vocal folds can be seen from above.The client is asked to produce a continuous vowel sound (i.e. /i/) to visualize the vocal folds during motion. This method is easy to administer and cost effective. However, images are small and there is no permanent record of these images. In addition, it does not allow examination of normal speech since the mirror in the mouth prevents the individual from speaking (Williamson, 2008).
-Rigid (oral) Laryngoscopy:
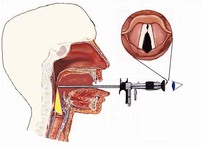
This method is in a way similar to the mirror laryngoscopy because the instrument is placed in the patient's mouth towards the back of the throat, however with this method, there is a lens at the end of the rod which is able to send images of the vocal folds to a camera. This method provides a better view of the vocal folds then the mirror technique and enables the clinician to save the images and enlarge them for easier viewing. On the other hand, since the rod is in the patient's mouth, the vocal cords cannot be assessed during connected speech and can only be assessed while sustaining a vowel or at rest (Williamson, 2008)
-Flexible Nasendoscopy:
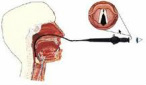
A narrow, flexible, fiberoptic cable with a camera attached is inserted into the nose to a position at the back of the throat above the vocal folds. Local anaesthetic nasal spray is often used to minimize discomfort. The advantage of this technique is that the vocal folds can be viewed during normal speech and singing since there is no instrument in the mouth to prevent this. Images can be saved to a computer for viewing and processing. Most children will tolerate this procedure relatively well. (Williamson, 2008)

-Video Stroboscopy: since the vocal folds vibrate so quickly, it is not possible to see their individual movements, but with the aid of a stroboscope, which can be fitted to either a rigid endoscope or to a flexible nasendoscope, the vibratory cycles of the vocal folds can be viewed as if they have been slowed down or made to stand still. A stroboscope emits flashes of bright light which can be coordinated with the frequency of vibrations of the vocal folds. This form of laryngoscopy is unique from the others because it allows for the examination of vocal fold vibratory behavior (Williamson, 2008).
The following video is of a child receiving a flexible nasendoscopy. The process is being described throughout the video and note how well the child is tolerating it. This child is receiving this procedure for hypernasality but the procedure is the same for vocal hyperfunction as well.
The following video is of a child receiving a flexible nasendoscopy. The process is being described throughout the video and note how well the child is tolerating it. This child is receiving this procedure for hypernasality but the procedure is the same for vocal hyperfunction as well.
Typically, both the child and caregiver will have a great deal of anxiety regarding any of these procedures. Here are some tips that both SLPs and parents can implement to help reduce the anxiety and fear that children might feel about the experience:
With children, the basic rule of thumb is to take everything calmly and slowly (Willamson, 2008), so that they will be relaxed during the procedure. If the child is relaxed, then the clinician will be able to obtain the best possible images (Theis, 2010).
- Explain the process – “The procedure is called laryngoscopy /nasendoscopy. An Ear Nose and Throat doctor is going to look at your voice box. The doctor will tell the Speech Pathologist what your voice box looks like and how it is working when you speak”.(La Trobe Communication Clinic, 2012).
- Involve the parent/caregiver to take part (La Trobe Communication Clinic, 2012).
- Show the child the equipment involved so that they don't feel threatened by it. Children will typically enjoy viewing things through the endoscope cameras such as their hair, buttons, shoe laces, etc. (Williamson, 2008).
- Meet the ENT or otolaryngologist beforehand.(LaTrobe Communication Clinic, 2012).
- Watch videos of the procedure (LaTrobe Communication Clinic, 2012).
With children, the basic rule of thumb is to take everything calmly and slowly (Willamson, 2008), so that they will be relaxed during the procedure. If the child is relaxed, then the clinician will be able to obtain the best possible images (Theis, 2010).
Research compiled by Miriam Klein, 2012.
